Agenda เอกราช อร ยะช ยพาณ ชย. - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 9/6/2016
|
|
|
- Bertha Grant
- 5 years ago
- Views:
Transcription

1 6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 1


2 Cardiovascular system 1. What is the heart? 2. What is the function of the heart? 2

3 The cardiovascular system Cardiac output (CO) The blood flow thru the heart in 1 minute L/min Stroke volume x Heart rate Intrinsic heart mechanics properties Preload // Contractility // Afterload What is preload? 3


4 1 Preload


5 Frank-Startling Mechanism SV Preload Preload: Cellular level 5
6 Preload in clinical A load to the contractile unit before contraction A load = Molecular z-z line contractile protein Cellular myocardial cell length Heart Wall stress LV end diastolic pressure --- LVEDP LV end diastolic volume --- LV size RA pressure --- JVP Volume status What is afterload? 6

7 Afterload Afterload SV Afterload 7

8 Afterload in Clinical A load that the heart has to contract against o Systolic blood pressure o Systolic vascular resistant o vaso-constriction 8
9 What is shock? What is shock? The clinical syndrome from various causes that result in damages due to inadequate global tissue perfusion. Inadequate O2 delivery Usually have hypotension (MAP < 60 mmhg) Lead to a vicious cycle, due to Organ protective mechanism Cellular dysfunction functional and structural change. multiple organ failure and death. Adapt from harrison principles of internal medicine 18th edition 9
10 HYPOTENSION SHOCK Hypoperfusion: Cellular responses ATP depletion Aerobic to anaerobic Abnormal membrane function Cell dysfunction, swelling, death Inflammatory response Hematologic response 10
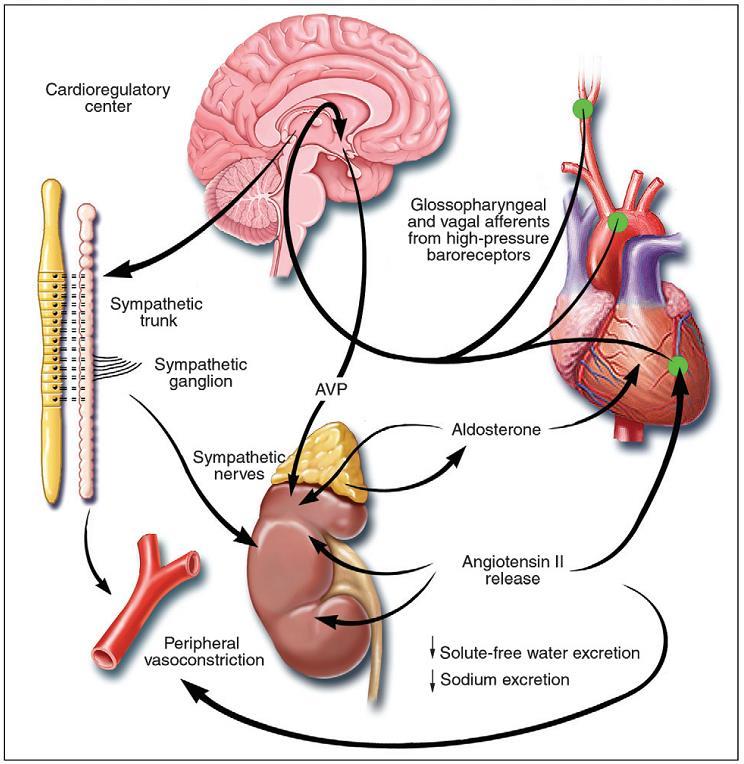
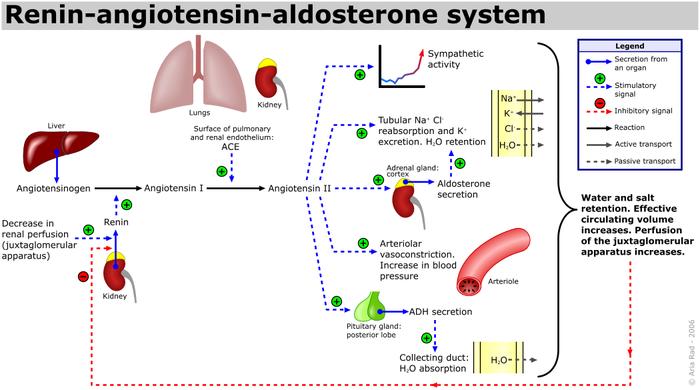
11 Hypoperfusion: Autonomic responses Sympathetic nervous system Baroreceptor, adrenal gland NE, epinephrine, dopamine, and cortisol release Vasoconstriction, HR, contractility, BP Renin-angiotensin-aldosterone system Water and Na absorption, vasoconstriction blood volume and BP ADH (vasopressin), cortisol, Multi organ dysfunction Renal failure Acute kidney injury Liver failure Ischemic hepatitis, shock liver DIC Respiratory distress or failure Cardiac depression 11

12 How many type of shock are there? 12

13 NEJM 2013 Type of shock Type of Shock Preload CO Afterload Cause Hypovolemic Cardiogenic Distributive Other type of shocks: Hypoadrenal, neurogenic, obstructive 13
14 Type of shock Type of Shock Preload CO Afterload Cause Hypovolemic Cardiogenic Distributive Other type of shocks: Hypoadrenal, neurogenic, obstructive Type of shock Type of Shock Preload CO Afterload Cause Hypovolemic Cardiogenic Distributive Blood or fluid loss (internal, external) Acute MI, acute HF Arrhythmia, cardiac tamponade pulmonary emboli Septic, anaphylaxis, inflammation, toxin Other type of shocks: hypoadrenal, neurogenic, obstructive 14
15 Type of shock JVP Central venous pressure Pulmonary capillary pressure Sign of hypovolumia Type of Shock Preload CO Afterload Cause Hypovolemic Cardiogenic Distributive Blood or fluid loss (internal, external) Warm vs. cold skin paleacute MI, acute HF Arrhythmia, Systemic vascular cardiac tamponade resistant pulmonary emboli Septic, anaphylaxis, inflammation, toxin Other type of shocks: hypoadrenal, neurogenic, obstructive S&S symptoms of hypoperfusion mental status Tachycardia BP urine cold skin Cr, Lactic acid. 15
16 Treatment Recognize shock Reverse the cause(s) In a timely fashion Support and prevent further end organ damage Restore perfusion ICU: Invasive monitor: Arterial line, foley cath, PA catheter (Swann-Ganz) Ventilation support: O2 support, Mechanical Ventilator/ Endotracheal tube Fluid resuscitation: Crystalloid > colloid. Cardiogenic shock Hemodynamic support: Inotrope, pressor, VAD Epinephrine Action Usual dose C 1 A 2 Note mcg/kg/min 1 mg iv bolus q 3 mins Norepinephrine mcg/kg/min Low dose = more. (like dobutamine) High dose = more. (like norepi) Use: ACLS, anaphylaxis, S/E: splanchnic vasoconstrict. Potent vasoconstriction. Moderate CO. HR effect (reflex bradycardia from increased MAP. Use: Septic shock. Dopamine Low Moderate High DA DA DA mcg/kg/min 2-10 mcg/kg/min mcg/kg/min Precursor to norepi but less, more effect. Dose-dependent effects. Dose is varied pt to pt. Use: Septic shock, 2 nd -line alternative to norepinephrine. Dobutamine 1 2 ( 1) 2-20 mcg/kg/min Milrinone PDE inh mcg/kg/min Isoproterenol mcg/min Phenylephrine mcg/kg/min 0 Not a vasopressor. Inotrope with a vasodilation. The net effect = CO + SVR, may not BP. Use: HF, cardiogenic. Similar to dobutamine more vasodilator, PA Use: HF, cardiogenic. Prominent chronotropic. Prominent vasodilation. Use: Bradycardia Pure vasoconstriction. May decrease SV. Vasopressin V unit/min 0 Pure vasoconstriction. Use: 2 nd -line in refractory vasodilatory shock.. S/E: coronary, mesenteric ischemia, skin necrosis. Na and pulm vasoconstriction 16
17 Sample A 55 yo M with hx of HTN, DM presents with crushing substernal CP, diaphoresis, hypotension, tachycardia and cool, clammy extremities An 81 yo F from a nursing home presents to the ED with altered mental status. She is febrile to 39.4, hypotensive with a widened pulse pressure, tachycardic, with warm extremities A 68 yo M with hx of HTN and DM presents to the ER with abrupt onset of diffuse abdominal pain with radiation to his low back. The pt is hypotensive, tachycardic, afebrile, with cool but dry skin N Engl J Med 2013; 369:
18 Cause of Hypovolemic Shock Non-hemorrhagic Vomiting Diarrhea Bowel obstruction, pancreatitis Burns Neglect, environmental (dehydration) Hemorrhagic GI bleed Trauma Massive hemoptysis AAA rupture Ectopic pregnancy, post-partum bleeding Cause of Septic shock Another lecture by it self Most common type of shock Hypoperfusion + infection + 2 SIRS (systemic inflammatory response syndrome) criteria S&S of hyperferfusion Temp > 38 or < 36 C HR > 90 RR > 20 WBC > 12,000 or < 4,000 Plus the presumed existence of infection 18

19 Sepsis Cardiogenic shock Hypoperfusion due to low cardiac output Low BP, high PCWP SBP < 90 mmhg CI < 2.2 L/m/m 2 PCWP > 18 mmhg 50% mortality rate 19


20 Pathophysiology Cardiac dysfunction Vicious cycle relaxation SV, Systemic flow contraction LVEDD, PCWP preload Pulmonary edema Hypoxia ischemia Coronary flow ischemia afterload Systemic hypopurfusion 20


21 Heart failure 21



22 Definition of HF 1. A syndrome caused by cardiac dysfunction 2. Leads to circulatory abnormalities and neurohormonal abnormality 3. Resulting in typical symptoms of Congestion Poor perfusion a. Common pathway from any causes b. Progressive, vicious cycle c. Systemic maladaptation 1 LVEDP dysfunction 2 Circulatory Abnormalities Neurohormonal abn. 3 Typical symptoms Dyspnea fatigue swelling 22

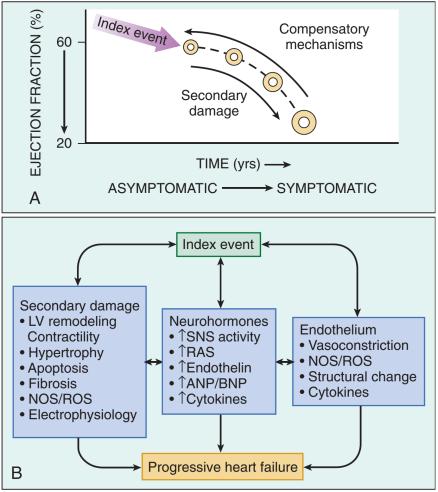
23 Cause of HF Circulation. 2013;128:e240-e327. Pathophysiology 23
24 24

25 J Am Coll Cardiol 2009;54:

 HJ reflux, ascites,")
26 Stage of HF S&S of HF Non specific, fatigue Dyspnea from increased breathing drive Reduction in exercise capacity (NYHA II-IV) Orthopnea, PND Edema, ascites, early satiety, N/V, confusion Apical shift, S3, S4, JVP, (+) HJ reflux, ascites, crepitation, edema 26
27 Treatment Self-care weight monitor, salt intake Diuretics to control symptoms Treatment To improve survival Betablocker ACE inhibitor or Angiotensin receptor blocker (ARB) Aldosterone blocker - spironolactone If channel inhibitor - Ivabradine Angiotensin receptor, neprilysin inhibitor(arni) Cardiac resynchronize therapy (special pacemaker) Implantable cardioverter Defibrillator End-stage HF Heart transplant Mechanical circulatory support Inotrope Palliative care - Valsartan/sacubitril 27


28 Circ Heart Fail.2008;1:63-71 Thank you 28
29 Back up slide Pressure volume Loop of the LV ESPVR (Ees) Ea A: MV close B: AV open C: AV close D: MV open Ees: end-systolic elastance (ESPVR: End systolic PV Relationship) EDPVR Ea: Arterial elastance EDPVR: End diastolic PV Relationship 29



: DDx type of shock,")
30 Control flow Murphy E. O2 content Control volume Control pressure Investigation Lab: shock Cr, AST/ALT, WBC, acidosis Troponin ECG: MI: ST elevation, Q wave, TW inversion CXR: pulmonary edema Echocardiogram: function, etiology Pulmonary catheter (Swan-Ganz): DDx type of shock, intracardiac pressure, CO Coronary angiogram 30
เอกราช อร ยะช ยพาณ ชย
 25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
Agenda. 1. Anatomy and physiology of the heart. 2. Pathophysiology of shock. 3. Pathophysiology of heart failure. 04-Sep-18
 เอกราช อร ยะช ยพาณ ชย Aekarach Ariyachaipanich, MD, FACC aekarach.a@chula.ac.th CVS 2 3000378 4.09.2018 Agenda 1. Anatomy and physiology of the heart 2. Pathophysiology of shock 3. Pathophysiology of heart
เอกราช อร ยะช ยพาณ ชย Aekarach Ariyachaipanich, MD, FACC aekarach.a@chula.ac.th CVS 2 3000378 4.09.2018 Agenda 1. Anatomy and physiology of the heart 2. Pathophysiology of shock 3. Pathophysiology of heart
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Shock Management. Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate. PDF created with pdffactory Pro trial version
 Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Means failure of heart to pump enough blood to satisfy the need of the body.
 Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Shock. Shao Mian Emergency Department,Zhongshan Hospital
 Shock Shao Mian Emergency Department,Zhongshan Hospital What is shock THE BEGINNINGS OF UNDERSTANDING: THE LATE 19TH CENTURY THE AGE OF REASON: 1890 1925 THE MODERN ERA: BLALOCK S EPIPHANY POSTMODERNISM:
Shock Shao Mian Emergency Department,Zhongshan Hospital What is shock THE BEGINNINGS OF UNDERSTANDING: THE LATE 19TH CENTURY THE AGE OF REASON: 1890 1925 THE MODERN ERA: BLALOCK S EPIPHANY POSTMODERNISM:
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the
 Objectives At the end of the session the") Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Unit 4 Problems of Cardiac Output and Tissue Perfusion
 Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
Unit 4 Problems of Cardiac Output and Tissue Perfusion Lemone and Burke Ch 30-32 Objectives Review the anatomy and physiology of the cardiovascular system. Identify normal heart sounds and relate them
LeMone & Burke Ch 30-32
 LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
LeMone & Burke Ch 30-32 2 Right side- Low oxygenation Low pressure Light workload Goes toward the lungs Left side High oxygenation Thick walled high pressure Heavier workload Carries oxygenation blood
Bachelor of Chinese Medicine Shock
 BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
BCM Year 2 Dr. Irene Ng Jan 28, 2003 9:30 am 1:00 pm Rm 004 UPB Bachelor of Chinese Medicine 2002 2003 Shock Learning objectives Be able to: know the definition of shock know the classification and causes
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H
 HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Failure of the circulation to maintain Tissue cellular. Tissue hypoperfusion Cellular hypoxia SHOCK. Perfusion
 Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Circulatory shock. Types, Etiology, Pathophysiology. Physiology of Circulation: The Vessels. 600,000 miles of vessels containing 5-6 liters of blood
 Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pediatric Shock. National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford
 Pediatric Shock National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford Pre-Topic Questions 1. Why is it important to identify the stage
Pediatric Shock National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford Pre-Topic Questions 1. Why is it important to identify the stage
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Case I: Shock. A) What additional history would you like from the nursing home staff, patient s chart, and ambulance team?
 What additional history would you like from the nursing home staff, patient s chart, and ambulance team?") Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
Case I: Shock It is your first night of call during your subinternship month, and you are asked by your resident to evaluate a patient in the emergency room. The patient is a 85yo female with a history
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
BIOL 219 Spring Chapters 14&15 Cardiovascular System
 1 BIOL 219 Spring 2013 Chapters 14&15 Cardiovascular System Outline: Components of the CV system Heart anatomy Layers of the heart wall Pericardium Heart chambers, valves, blood vessels, septum Atrioventricular
1 BIOL 219 Spring 2013 Chapters 14&15 Cardiovascular System Outline: Components of the CV system Heart anatomy Layers of the heart wall Pericardium Heart chambers, valves, blood vessels, septum Atrioventricular
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Objectives. Objectives. Shock. Objectives. Cardiac output. Review of Blood Flow and Perfusion. Review the components of perfusion
 Objectives Shock Review the components of perfusion Cardiac output Perfusion at the capillary level Perfusion and cellular metabolism Aerobic metabolism and energy production Objectives Identify the stages
Objectives Shock Review the components of perfusion Cardiac output Perfusion at the capillary level Perfusion and cellular metabolism Aerobic metabolism and energy production Objectives Identify the stages
SHOCK. Voravit Chittithavorn. Cardiovascular Thoracic Surgery Department of Surgery
 SHOCK Voravit Chittithavorn Cardiovascular Thoracic Surgery Department of Surgery Shock: Introduction Cellular Injury Multiorgans Dysfunction Irreversible Processing Unbalance Supply vs Demand Perfusion
SHOCK Voravit Chittithavorn Cardiovascular Thoracic Surgery Department of Surgery Shock: Introduction Cellular Injury Multiorgans Dysfunction Irreversible Processing Unbalance Supply vs Demand Perfusion
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Tissue oxygenation is dependent upon, cardiac output, hemoglobin saturation and peripheral micro circulation.
 Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
SHOCK PATHOPHYSIOLOGY
 SHOCK PATHOPHYSIOLOGY shock Shock is a condition in which the cardiovascular system fails to perfuse tissues adequately An impaired cardiac pump, circulatory system, and/or volume can lead to compromised
SHOCK PATHOPHYSIOLOGY shock Shock is a condition in which the cardiovascular system fails to perfuse tissues adequately An impaired cardiac pump, circulatory system, and/or volume can lead to compromised
Definition. Emergency Treatment 11/13/13. Pathophysiology of circulatory shock. Characteristics of circulatory shock. Clinical features of shock
 Definition Pathophysiology of circulatory shock! Inadequate perfusion (oxygen supply) of tissues, resulting in:! Organ dysfunction! Cellular and organ damage And if not quickly corrected! Death Dr Badri
Definition Pathophysiology of circulatory shock! Inadequate perfusion (oxygen supply) of tissues, resulting in:! Organ dysfunction! Cellular and organ damage And if not quickly corrected! Death Dr Badri
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure. Part I: Etiology and Pathophysiology of Heart Failure
 A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
A Guide to the Etiology, Pathophysiology, Diagnosis, and Treatment of Heart Failure Dr Badri Paudel GMC Part I: Etiology and Pathophysiology of Heart Failure Heart Failure (HF) Definition A complex clinical
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Ventriculo-arterial coupling and diastolic elastance. MasterclassIC Schiermonnikoog 2015
 Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Physiology #14. Heart Failure & Circulatory Shock. Mohammad Ja far Tuesday 5/4/2016. Turquoise Team. Page 0 of 13
 45 Physiology #14 Heart Failure & Circulatory Shock Mohammad Ja far Tuesday 5/4/2016 Turquoise Team Page 0 of 13 Heart Failure: It s a condition in which the heart can t perform its function properly;
45 Physiology #14 Heart Failure & Circulatory Shock Mohammad Ja far Tuesday 5/4/2016 Turquoise Team Page 0 of 13 Heart Failure: It s a condition in which the heart can t perform its function properly;
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Blood pressure. Formation of the blood pressure: Blood pressure. Formation of the blood pressure 5/1/12
 Blood pressure Blood pressure Dr Badri Paudel www.badripaudel.com Ø Blood pressure means the force exerted by the blood against the vessel wall Ø ( or the force exerted by the blood against any unit area
Blood pressure Blood pressure Dr Badri Paudel www.badripaudel.com Ø Blood pressure means the force exerted by the blood against the vessel wall Ø ( or the force exerted by the blood against any unit area
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
PEDIATRIC SHOCK 10/9/2014. Objectives. What is shock? By the end of this presentation, the learner will be able to:
 PEDIATRIC SHOCK Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CMS, CEN, CNRN, CPNP Education Specialist-LRM Consulting Nashville, TN Objectives By the end of this presentation, the learner will be able to:
PEDIATRIC SHOCK Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CMS, CEN, CNRN, CPNP Education Specialist-LRM Consulting Nashville, TN Objectives By the end of this presentation, the learner will be able to:
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1
 Lecture 14 Cardiovascular control mechanisms p. 1") BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Improving Transition of Care in Congestive Heart Failure. Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare
 Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya
 Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National University Canberra Hospital, Australia Inotropes
Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National University Canberra Hospital, Australia Inotropes
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac